Previous Cases (Home Page)
Intro
ED Visit
ED Bounceback
Referral Hospital
Autopsy
Expert Witness Opinions
Legal Outcome
Medical Review
Documentation Review
For this case’s medical review, we will use the opinions of the expert witnesses to help guide the discussion. The crux of the case essentially comes to down to whether or not the patient’s presentation prospectively warranted further medical or traumatic workup. There is a range of risk tolerance among EM doctors that falls within the standard of care, but being too risk-tolerant can fall outside of the acceptable range. Being too risk-averse wastes resources, irritates colleagues, slows the department, and may not ultimately provide any further protection. After all, bad outcomes are going to happen to all ER doctors eventually, no matter how smart you are or how well you practice.
The first expert witness (for the plaintiff) makes several assertions about appropriate care for this patient. The first is in regards to not developing an appropriate differential that would include closed head injury, and the failure to get a CT scan. In regards to trauma indication for head CT, there are some useful criteria to help decide which patients need a CT scan.
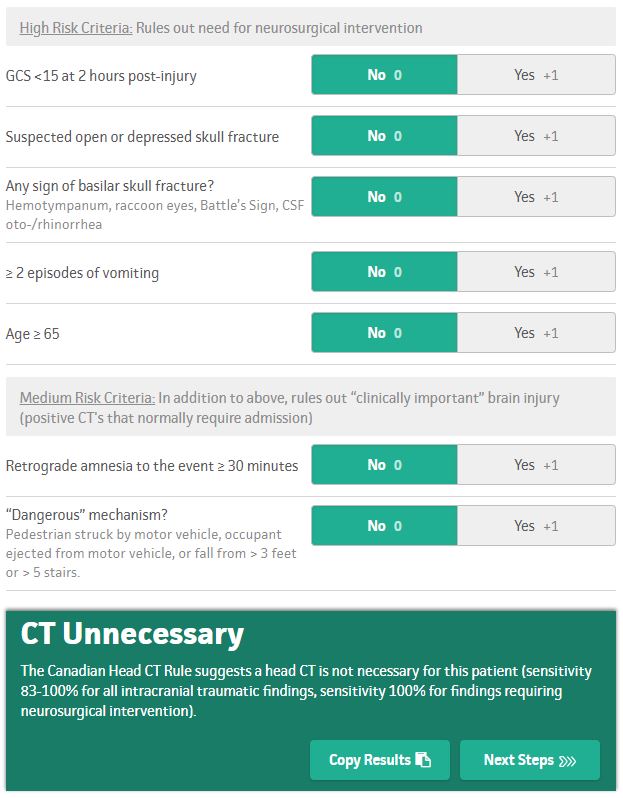
According to these criteria, there is no indication for head CT in this case (at least in regards to traumatic injuries). The patient had vomited previously, but this was prior to the accident, and the physician had documented GCS 15 at the original visit, and no obvious signs of trauma.
The question then becomes if there is another indication for ordering a head CT. EMS and police documentation clearly describe the patient as confused at the scene, but this could easily be explained by a concussion from the accident. Furthermore, a CT scan would not have identified meningitis. There was a small bleed 2 days later on CT scan (that did not contribute directly to his death and would likely have not required surgical intervention), but this may not have even been present even if he was scanned at the original visit.

The first expert witness makes another claim that neurology or neurosurgery should have been consulted. Any EM physician knows that consulting either of these services for a patient who was slightly confused, had nausea and vomiting for a few days, and crashed their car would be very atypical. Even if the EM physician had gotten a consult, the recommendations may not have been any different. And furthermore a recommendation for observation in the hospital would have required convincing a hospitalist or trauma surgeon to admit the patient, which depending on the agreeableness of the admitting physician, may not have been possible. Assuming the patient was admitted to the hospital, it is not even clear if this would have changed the outcome. If the patient did not have any change in his condition by the following morning, there is a high likelihood he would have been discharged. His mental status did not worsen until 2 days after the the ED visit, and he may have been discharged back home prior the development of worsening mental status.
Another opinion from the 1st and 2nd expert witnesses is that blood cultures should have been drawn and antibiotics given. Obtaining blood cultures would not have been helpful at the time given that it can take several days to get a result. There has been significant work on using blood cultures in the ED, well-explained in this post from EM Docs. In regards to starting antibiotics, it is difficult to justify given the fact that he was only mildly tachycardic after arriving to the ED, and his heart rate improved significantly with fluids. While he may have met SIRS criteria, that fact alone is poor justification for ordering blood cultures and antibiotics given the high numbers of patients with SIRS criteria who do not have sepsis. This issue was raised by Expert Witness #2 and appropriately dismantled by Expert Witness #3, including the bizarre typos described SIRS criteria as “service” criteria. It is strange to hear an infectious disease physician advocate for giving antibiotics under these circumstances, a decision that would results in vast over-utilization of antibiotics and likely contribute to antibiotic resistance.
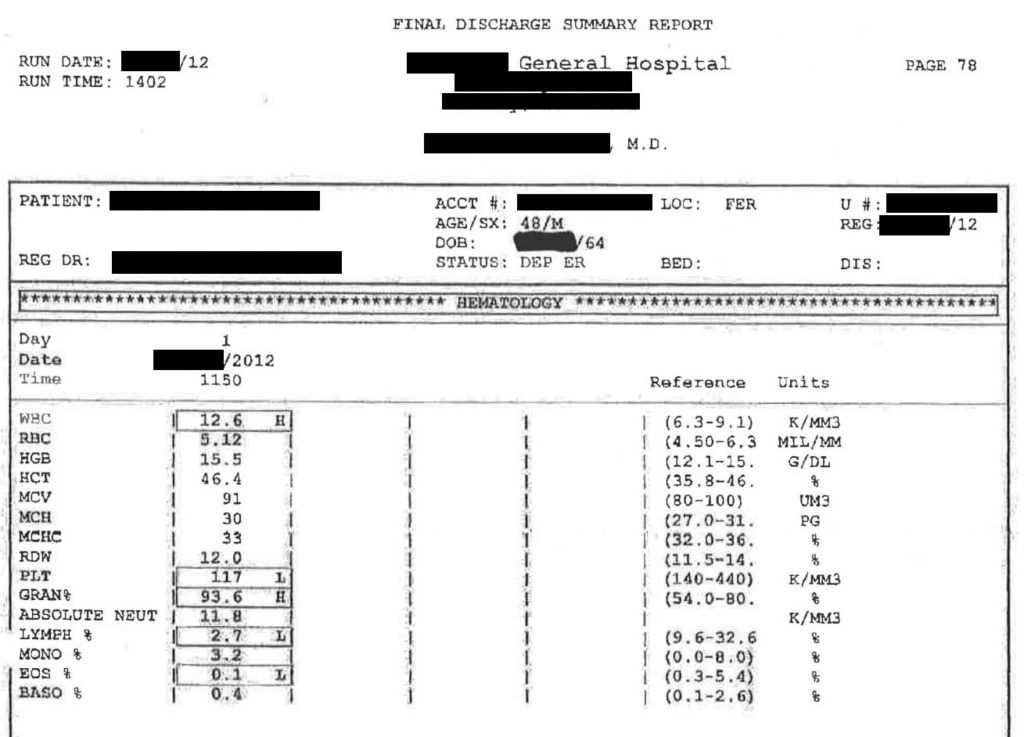
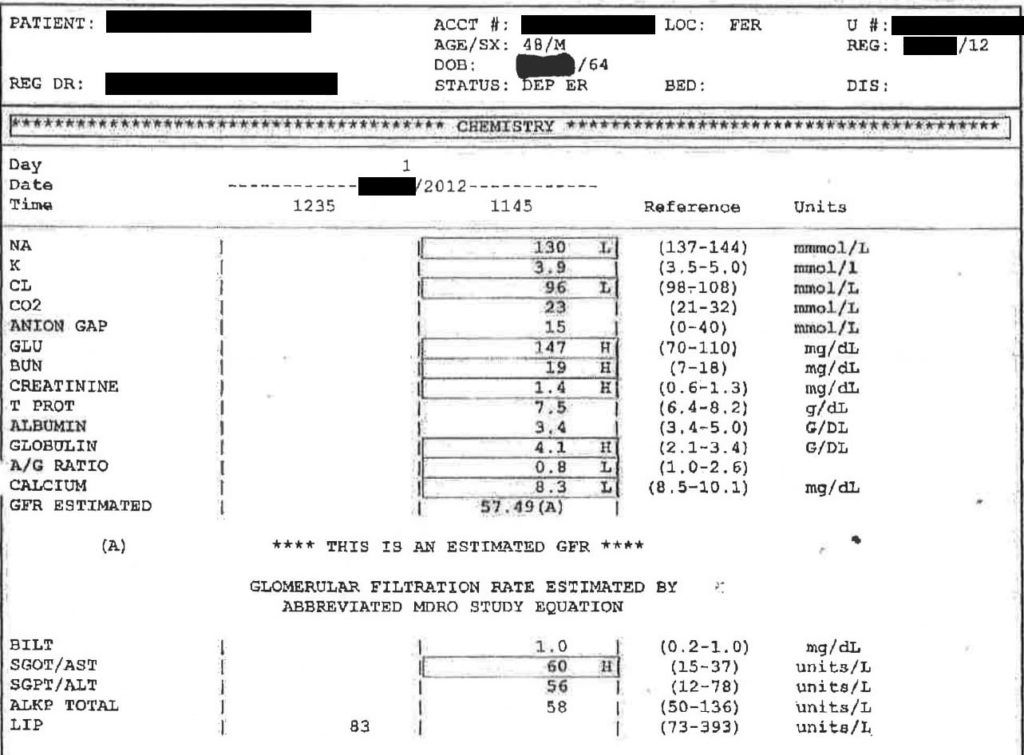
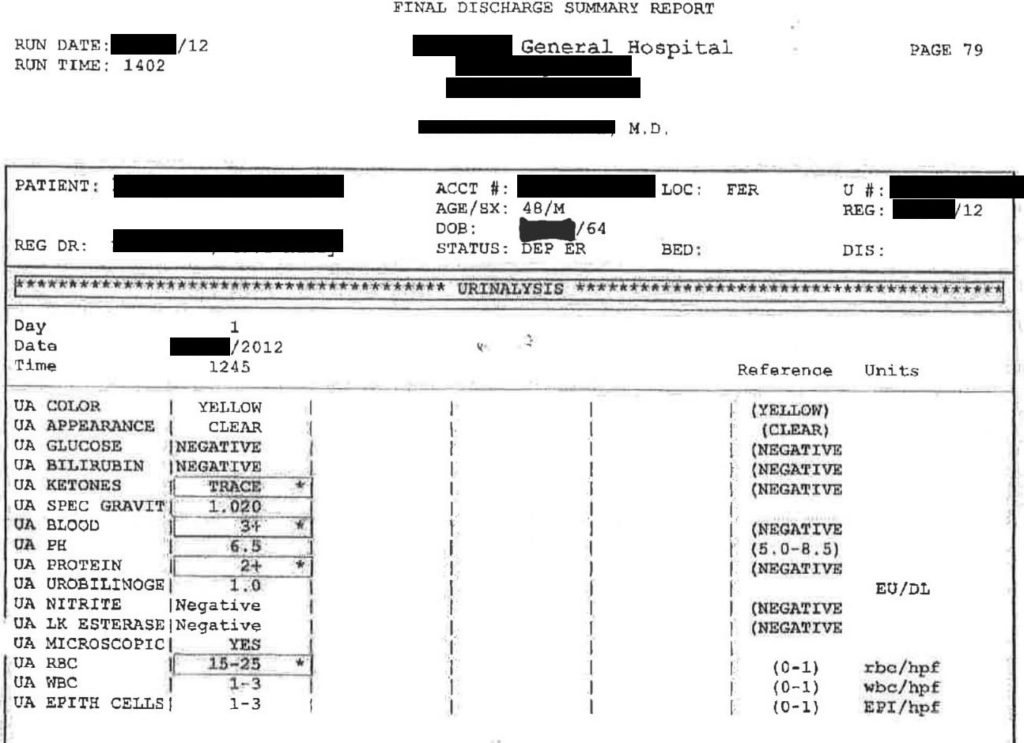
The patient had several lab abnormalities including slight leukocytosis and thrombocytopenia, and several mild electrolyte abnormalities. These are not unusual findings in patients after a MVC.
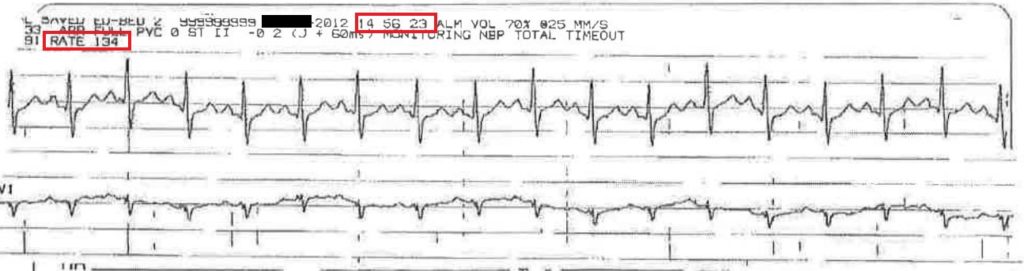
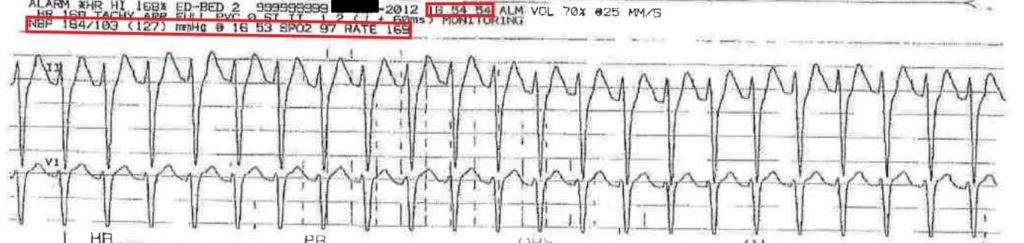
Another area of improvement is the receiving physician’s decision to give the patient adenosine. Unfortunately there are no rhythm strips from the referring hospital, but we do have a description of his rhythm as a broad-based, irregular tachycardia. Recall that at the previous ED, his heart rhythm was initially narrow and regular, but as is heart increased, the morphology changed and the QRS widened:
Upon arrival to the receiving hospital, the patient’s heart rate is obviously a response to his underlying septic condition, not the primary etiology of any hemodynamic instability. The physician gave him a dose of adenosine, which would be more appropriate for SVT, a narrow complex, regular rhythm. The dose of adenosine came only about 15 minutes prior to his death. While adenosine has an extremely short half-life, the close timing between giving adenosine and the patient’s death is concerning. The exact circumstances of this specific case are difficult to determine because we do not have an EKG after arrival to the receiving hospital, but this blog post from Dr. Smith’s EKG blog does a great job of describing the general approach to wide complex, irregular rhythms.
One of the main learning points from this case is to always consider underlying medical illness as a cause of a trauma. This is especially apparent in the elderly population, where a traumatic fall can be the first presentation of serious underlying medical emergency. It is important to not focus solely on the trauma. The physician in the case was certainly aware of an underlying illness, but the relative importance of the underlying illness was difficult to appreciate given the overall benign test results and the patient’s young age.