Index Case 7
Ankle Injury
Testing and Treatment
Disposition
Billing
Return ED Visit
Outcome
Plaintiff Claims
Defense Response
Legal Outcome
Case Review
Documentation Review
The diagnosis of necrotizing fasciitis (NF) can be very challenging. It is one of the disease processes that can have very subtle findings initially, but can rapidly progress to critical illness.
Benign initial appearance
Often times, the initial history and exam appear consistent with cellulitis. Obvious cases of NF are easy to identify, but the vast majority of bad outcomes from this disease occur because the initial stages appear relatively benign. Even with a thorough workup and expert emergency medical care, it may be impossible to detect the disease.

Search for a unifying disease process
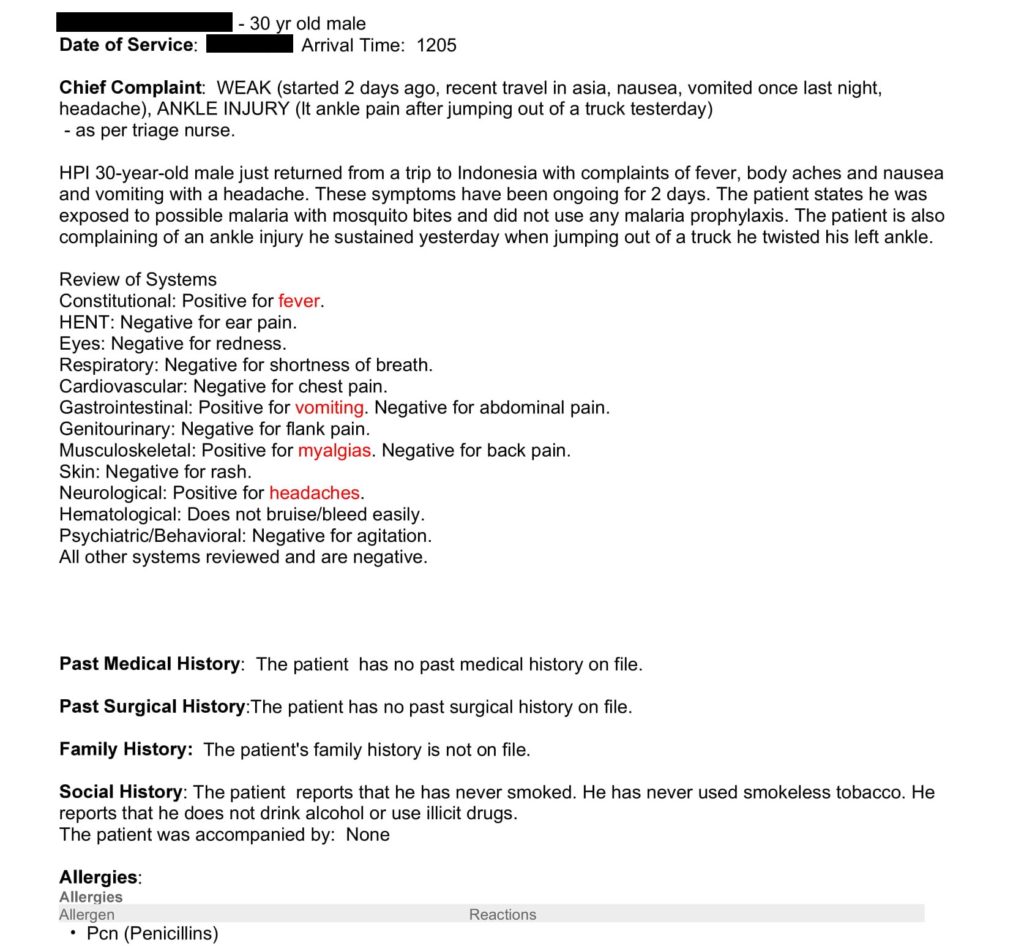
In this case, the initial presentation was very benign. At his initial presentation he had systemic symptoms (vomiting, myalgia, fever, headaches) in addition to his ankle pain. The EM physician did not cognitively link the ankle pain with the systemic symptoms. They were considered as two separate issues. When faced with a patient who has multiple varied symptoms, it is a wise exercise to consider what singular issue could be explaining all these symptoms.
In the physician’s defense, there seems to have not been any erythema, blistering, or other signs of skin infection at the ankle. Even if a connection had been made between a skin infection and systemic symptoms, it is not uncommon for cellulitis to cause this presentation.
Failure of Communication
A common theme in medical malpractice cases is a failure of communication at some point (see last month’s case where it seems that the physician did not realize that the patient had been anticoagulated). In this case, the physician seems to have been lacking the information that the patient had been hypotensive at the clinic prior to ED presentation. However, even with this information, there is a reasonable argument that the patient would still have been discharged. His blood pressure was completely normal in the ED. He was not tachycardic or febrile. Every EM doctor knows it would be tough to sell this admission to a hospitalist solely based on the fact that he had one hypotensive blood pressure in the clinic, especially with normal blood pressure in the ED. The oft ridiculed suggestion of ICU or discharge (but not floor admission) may be invoked: “If he’s that hypotensive he needs to go to the ICU, if he has normal vitals he should be discharged”.

Building Safe Systems and Institutional Malpractice
Questioning the patient about why they came to the ED may have revealed valuable information. It is amazing how a full conversation with a patient may fail to elicit a critical bit of information. Even when asked open-ended questions in a careful and thorough manner, the fact that they were referred to the ED may not be discovered. There are several possible solutions to this communication issue. Outpatient facilities sending patients to the ED should actively seek to make sure that the reason for ED referral is communicated. EDs may benefit from including this question in the standardized intake questioning. Building a system that makes these communication failures less likely will help EM physicians take excellent care of patients. The responsibility for building safe systems falls on the institution. Other examples of institutional failures complicated by poor individual decision-making include Case 1 (hospital did not have the right equipment to care for the patient) and Case 6 (hospital banned EM doctor from using appropriate medications).
Disease Progression
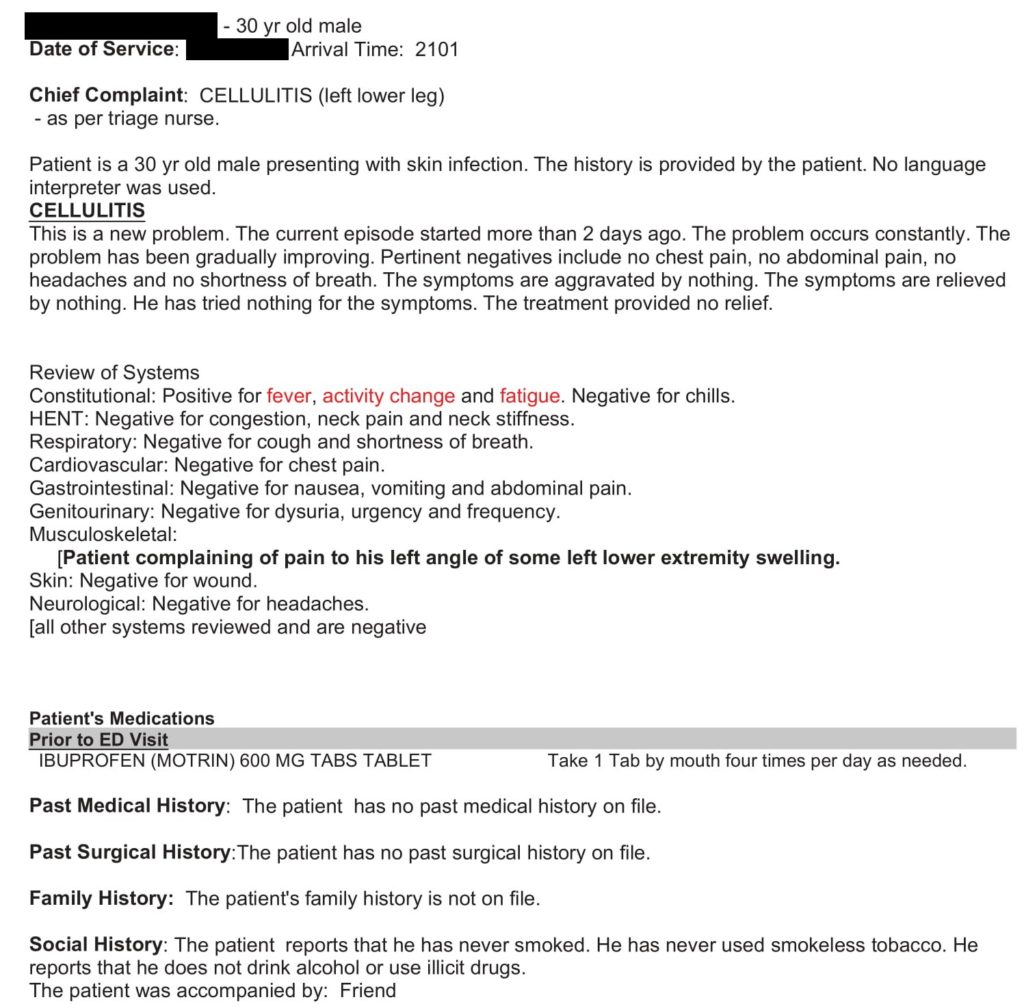
Another key factor in making the diagnosis of necrotizing fasciitis is that pain out of proportion to exam may be present. At the initial presentation, the patient did not have pain out of proportion. He had ankle pain that seemed consistent with an ankle sprain. However, on the return visit, he had developed worsening pain and swelling of the ankle. It was immediately identified as an infection by the triage nurse (chief complaint is listed as cellulitis).
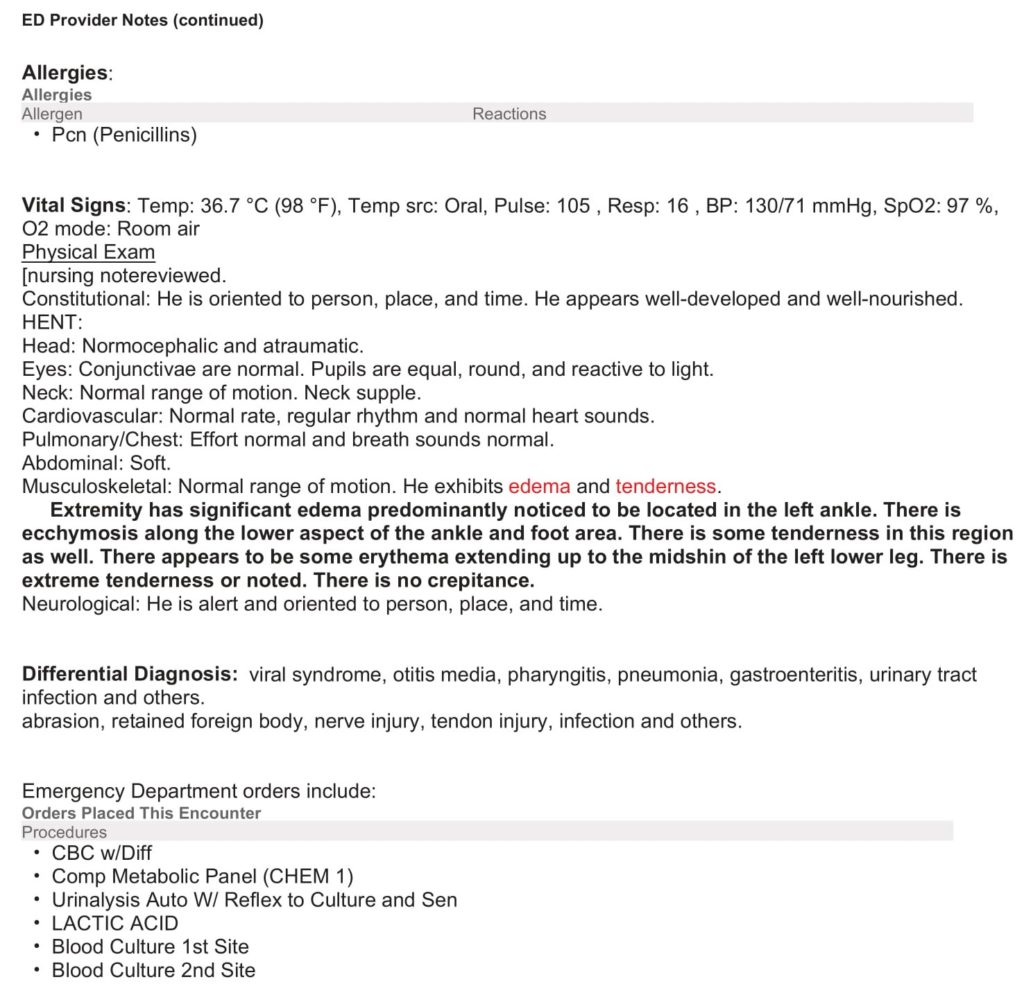
The note indicates erythema, echymosis, “extreme tenderness” and “significant edema”. These symptoms should trigger any EM doc to consider NF, but by no means do they clinch the diagnosis. Another key finding is crepitus, but it is only present in a minority of NF cases, and was absent in this case. Blistering is associated with worse outcomes, but was also not present in this case.
Source: http://www.nuemblog.com/blog/nec-fasc
Interestingly, the physician did actively consider necrotizing fasciitis. The statement “there is nothing on patient’s exam or history to assess that [necrotizing fasciitis] is present” is obviously false in hindsight, but he does modify this statement later.
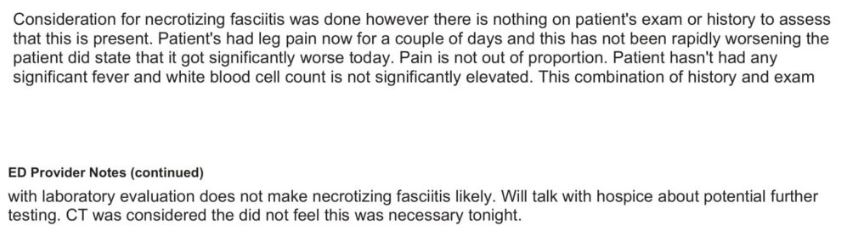
He states that “this combination of history and exam with laboratory evaluation does not make necrotizing fasciitis likely”, which is a much more appropriate statement than just dismissing it outright. The physician justifies this claim based on a few findings. First, he states that the pain was not rapidly progressing until today, which does not provide any support for conclusion that this is not NF. Second, the pain is described as not being out of proportion to exam, despite being described in the physical exam as “extreme tenderness”. This brings up the issue that “pain out of proportion” is an extremely subjective physical exam finding. There is no way to standardize this finding or make it reproducible. Third, the patient is noted to be afebrile and the WBCs are not significantly elevated. These findings are not sufficient to rule out NF.
Imaging in Cases of Possible Necrotizing Fasciitis
Plain films were obtained of the ankle at the initial ED visit. Plain films are helpful to rule out other issues, but are rarely helpful in the diagnosis of NF. The only way they are possibly helpful is if there is enough gas in the tissue to show up on xray, by which time the diagnosis is probably not subtle.
On the repeat visit, the physician notes that “CT was considered [but] did not feel this was necessary tonight”. There is evidence that CT is useful for ruling out NF. There is an argument to be made that this case would have been a good time to consider CT to assess for this diagnosis, as the physician considered that it was possible but felt it was unlikely.
The plaintiff’s attorney made claims that an MRI should have been performed. Unfortunately, the ED did not have access to an MRI scanner at the time, which is the case in most EDs. Obtaining an MRI for emergencies such as cauda equina syndrome or spinal epidural abscess (Case 2) are hard enough, let alone a scan of an extremity.
While imaging may be useful in necrotizing fasciitis, there are cases in which there is no subcutaneous air to detect, and imaging alone is insufficient to make the diagnosis.
Source: http://www.emdocs.net/misdiagnose-mismanage-necrotizing-fasciitis/
LRINEC score
The LRINEC score is a screening tool that was created by comparing cases of true necrotizing fasciitis to cases of severe cellulitis. It does require CRP testing, which is not in most typical ER workups but can be obtained in most EDs. It is an easy score to calculate, which makes it an easy target for diagnostic anchoring. Unfortunately, even a score of 0 is not sufficient to rule out the diagnosis.
Source: http://www.emdocs.net/necrotizing-fasciitis-pearls-pitfalls/