Recap: A 31 year old man presented to an ED with shortness of breath, chest pain, cough, and was found to be febrile, tachycardic, and tachypneic. He had an elevated D-dimer, negative lower extremity ultrasounds and normal chest xray. A CT was ordered but cancelled because he weighed more than the machine could tolerate. He was discharged and instructed to follow-up at another hospital if not improving after a few days.
Home Page
Post 1: Introduction
Post 2: Bad Outcome
Post 3: Legal Outcome
Post 4: Documentation Review
Post 5: Medical Review
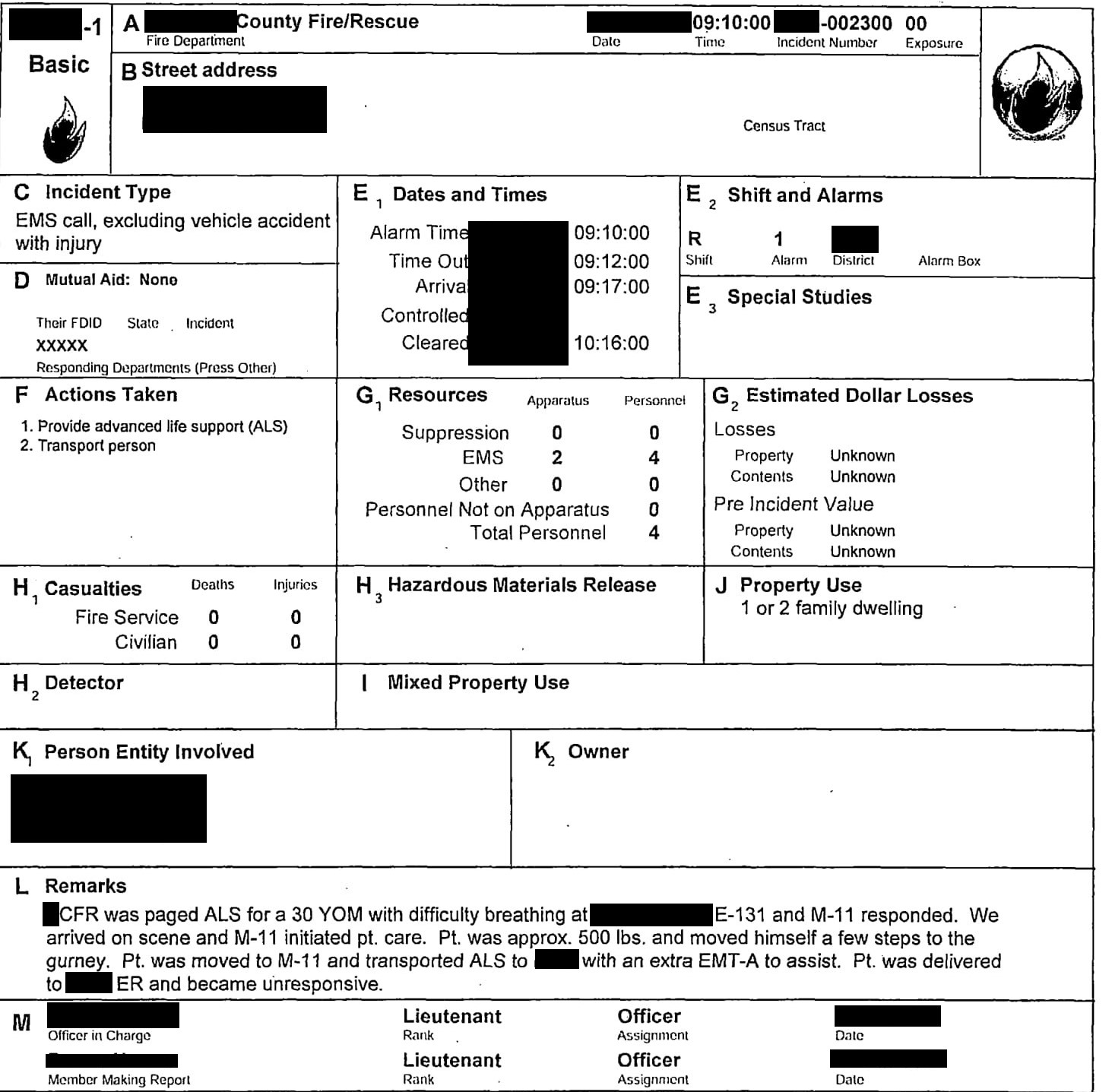
The man did indeed begin to improve, and several days later he was feeling much better. He was in the process of moving across the US, and took a long car trip to make it to his destination. Several weeks after the first visit, however, he began to again develop shortness of breath. He then passed out a few times at home, and the following day (18 days after the initial visit), his family called 911. The EMS run sheet is shown below.
Unfortunately, as the ambulance arrived to the ED garage, he became unresponsive and was found to be pulseless and apneic. This ED was in a completely different state, so no previous information was available. The treating physician had some basic information from EMS, and the patient’s wife once she arrived shortly after he coded. The patient underwent multiple rounds of chest compressions and epinephrine, and got pulses back a few times. An EKG reportedly showed a RBBB (EKG not included in the evidence for this case).
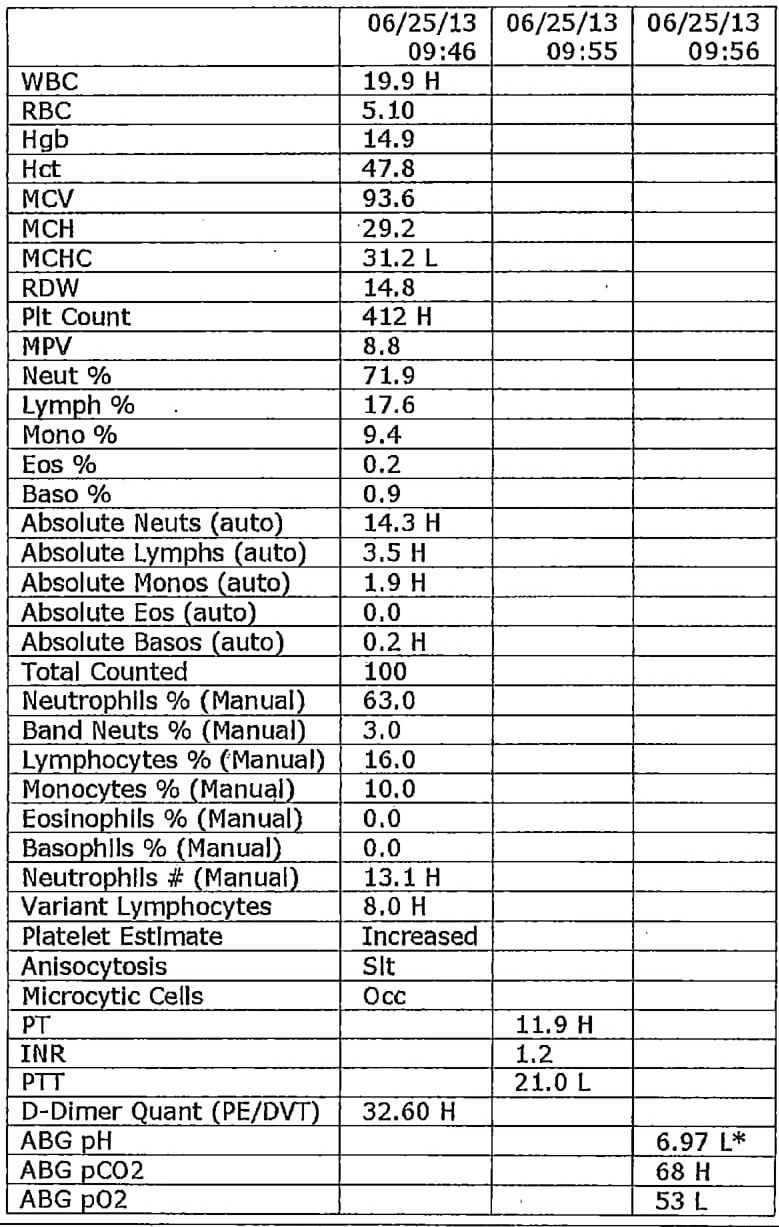
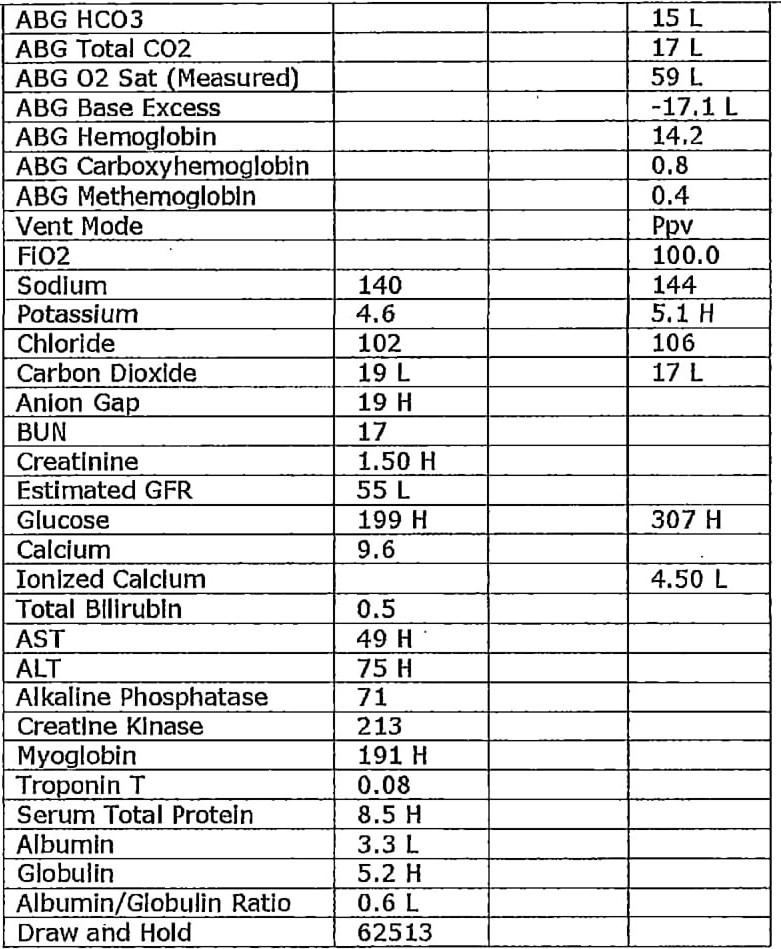
The doctor was able to get a fem stick and sent labs. The patient again had an elevated D-dimer, and a VBG showed an acidosis with pH < 7.
Unfortunately the patient again lost his pulse. Further rounds of CPR and epinephrine continued. He was also given 2 amps of bicarb. The rhythm was never shockable. ETCO2 ranged from 8-15 throughout the code. The physician performed a bedside ultrasound showing no cardiac contractility and no pericardial effusion, and ultimately the code was called about 30 minutes after his arrival.
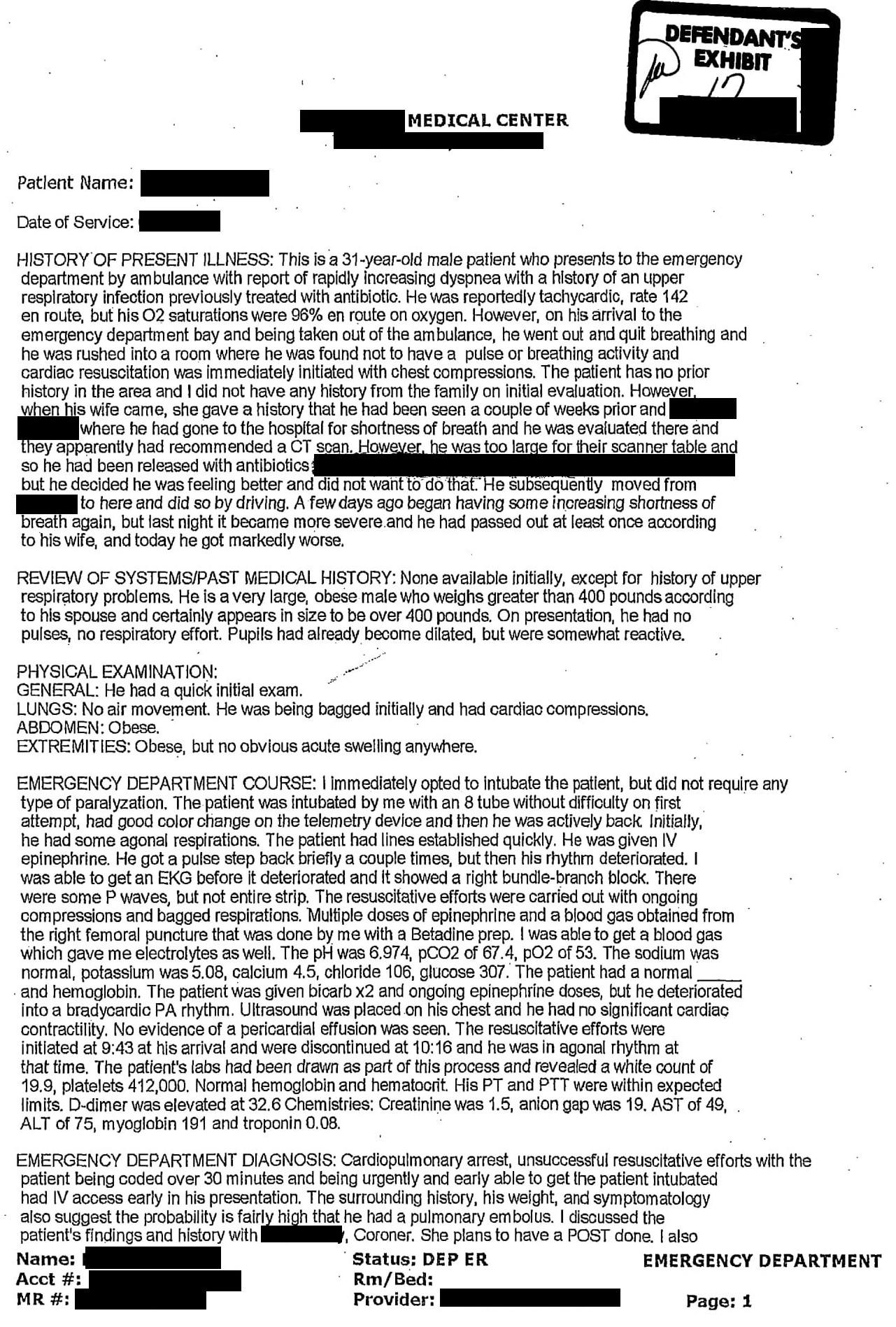
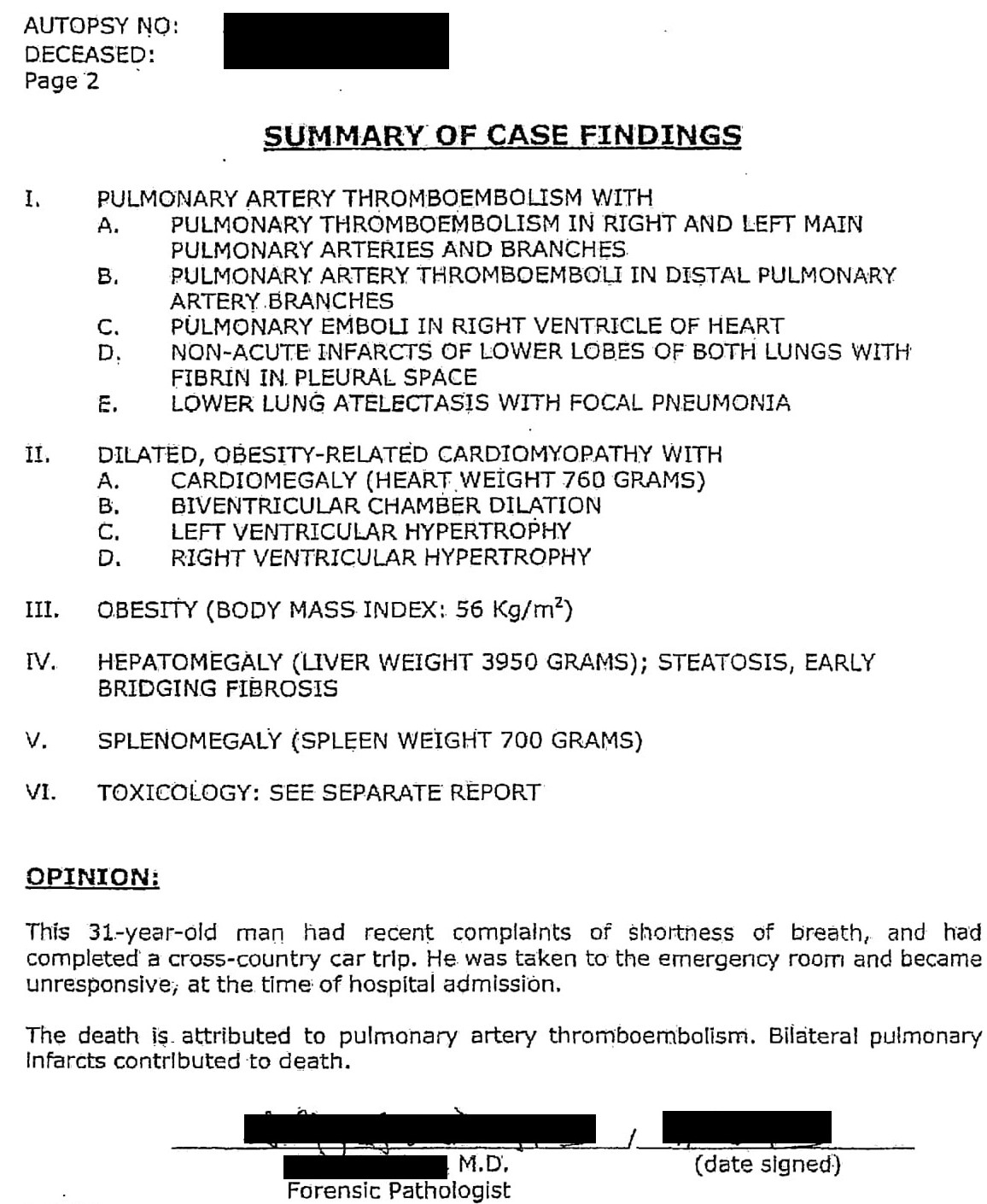
At the end of the note, the physician states that the case is strongly suspicious for PE, and that an autopsy will be done. Several days later, the autopsy is completed. The results confirm the diagnosis of PE, with clot found in both the right and left main pulmonary arteries, the right ventricle, and associated non-acute infarcts of both lungs. The final opinion states “the death is attributed to pulmonary artery thromboembolism”.
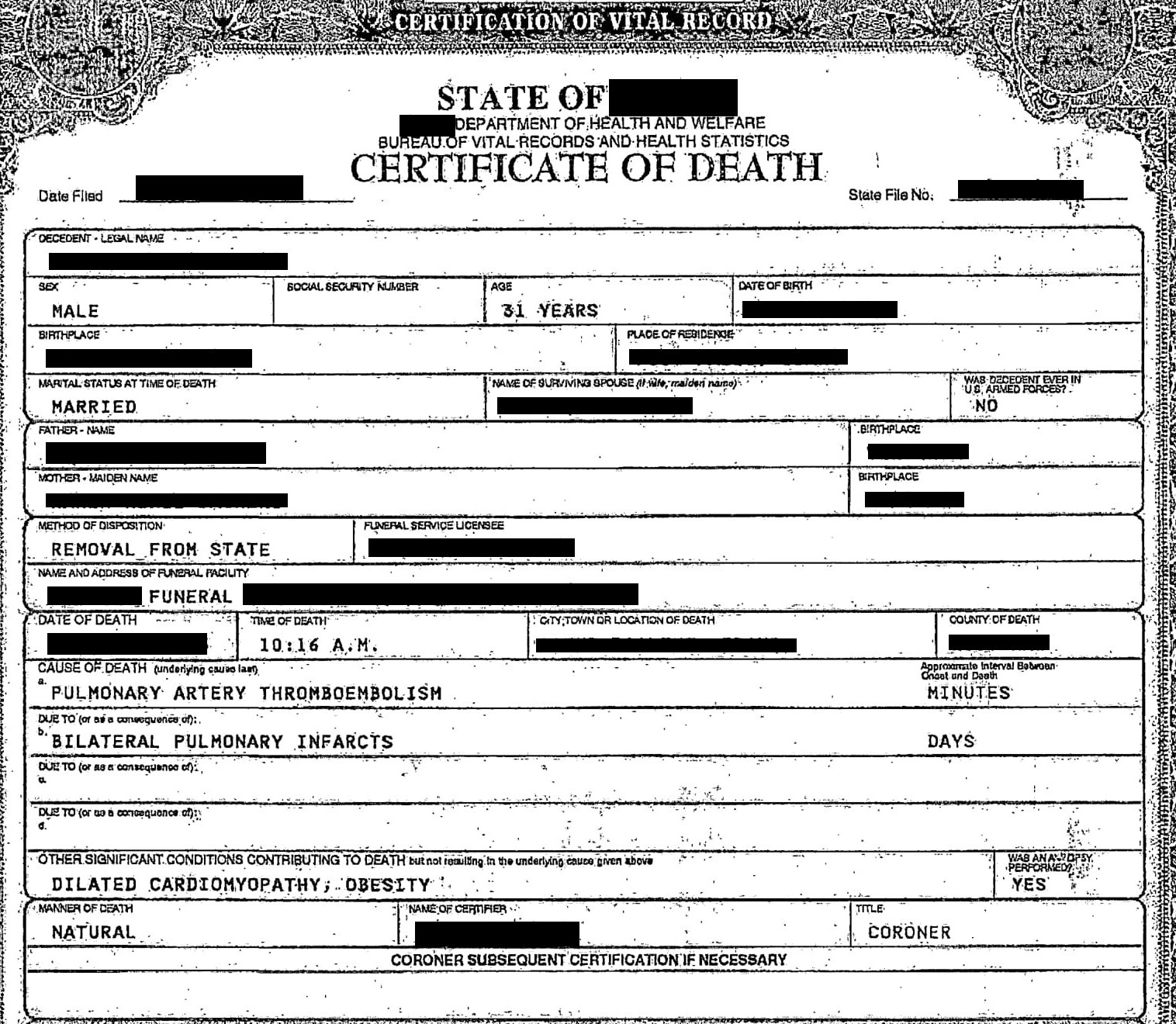
The death certificate is shown below.
To view the bill for the funeral, see below.