The documentation from the patient’s initial visit will be reviewed. In order to provide a standardized analysis, a Documentation Rubric is used to assess the documentation in each MedMalReviewer case. The most important part of the note for malpractice cases is the medical decision-making (MDM). While the rest of the note is important for billing and communicating with other clinicians, we will focus on the MDM.
The Rubric is used for grading documentation in hindsight. For help creating good notes while working clinically, see the Documentation Template.
This note scored 8/20 points.
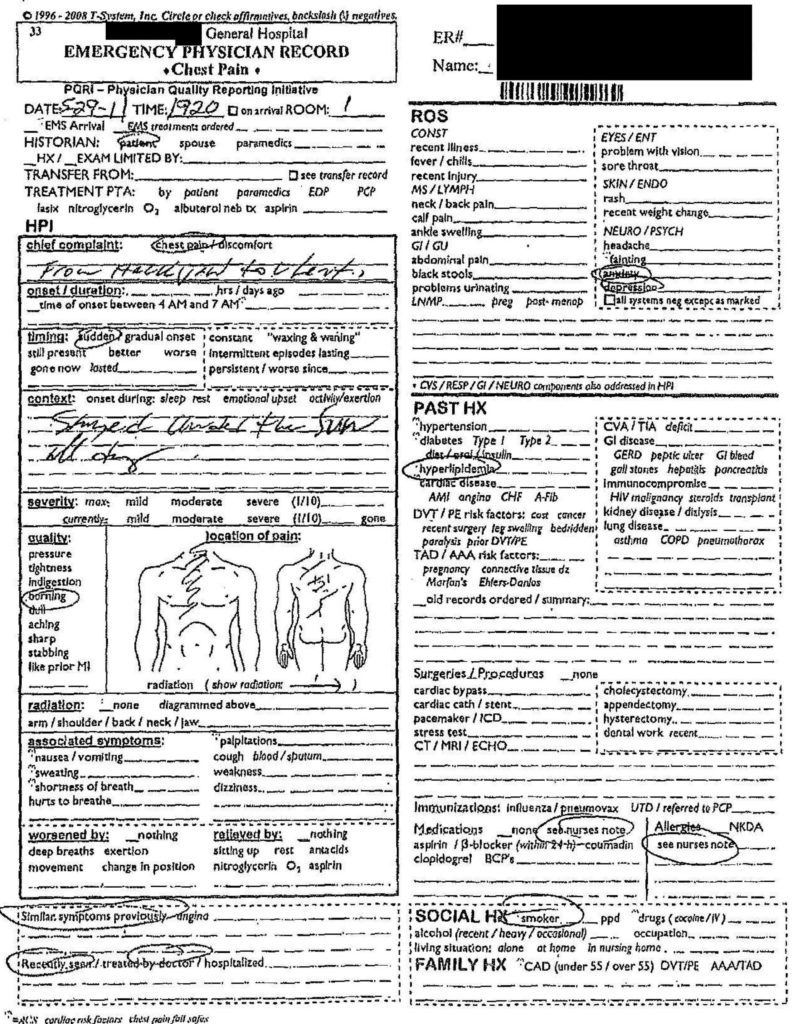
One of the challenges in this case is the fact that T-sheets were used for documentation. T-sheets help doctors write notes quickly, but they are notorious for containing almost no useful information if a chart has to be reviewed. They may be useful for very straightforward patients with simple medical issues and no comorbidities. Unfortunately this patient did not fall into that category.
Brief Overview: 0.5/2
It is useful to start the MDM with a basic overview about the patient’s presentation. This helps distill the history and exam into 1-2 sentences of relevant information.
This note unfortunately barely contains enough information to qualify as a documented history. The documentation of her risk factors is important in this case, and he seems to have either missed several of them or failed to document them.
Testing: 1.5/2
When the work-up is logical based upon a review of the patient’s history and presentation, no explanation is needed. However, when unusual testing is ordered, or typical testing is left out, it needs to be clearly explained.
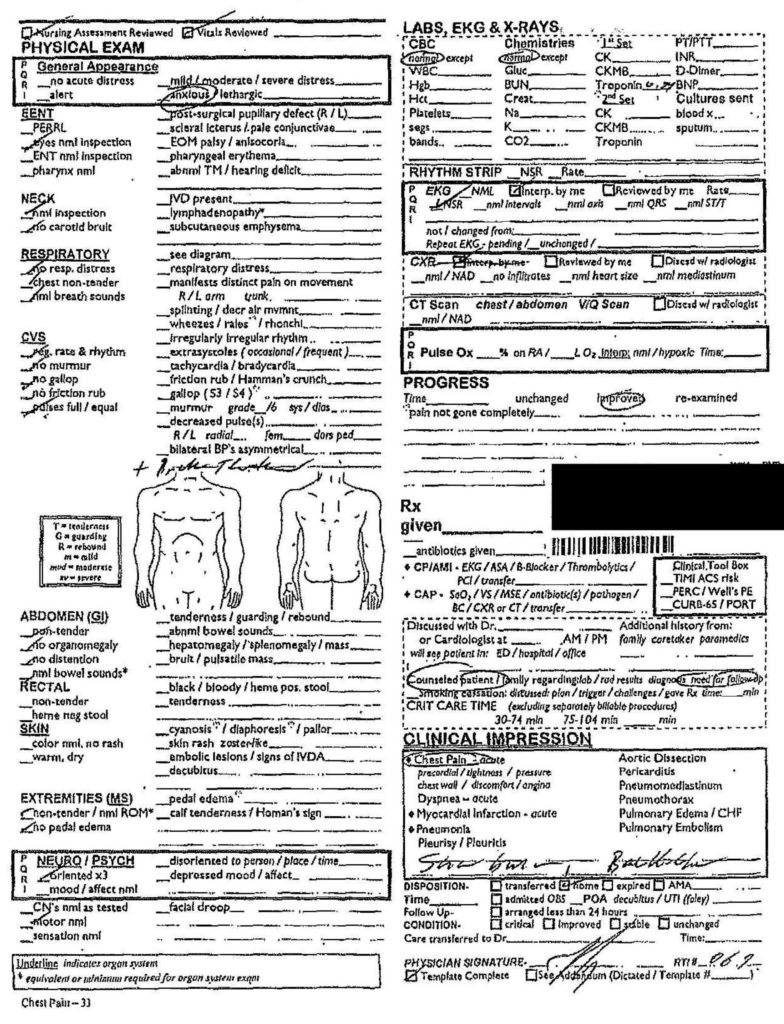
In this case, the physician ordered a fairly standard workup for a chest pain patient. The only issue for consideration is the chest x-ray. The court records do not contain any evidence that a chest x-ray was ordered, nor any radiology of an x-ray. However, his note includes a checkbox that indicates he looked at one. It is unclear if he actually got an x-ray and the court documents simply left it out, or if he erroneously checked this box.
Therapy: 2/3
The medications given to the patient included nitroglycerin, Toradol and normal saline. These tests are not particularly unusual for a patient with chest pain. What is unusual is the fact that the physician was worried about cardiac ischemia, and did not order aspirin. Explaining why he did not want to give a key medication for the very disease he was investigating would have been wise.
Points were not deducted because of the medical decisions (no aspirin) that were made, but because of a failure to adequately explain them. Doing something atypical is fine, but documenting why it was done is critical.
Differential: 2/8
The MDM is the most important section of a medical note. The differential is the most important section of the MDM. It is a good habit to document at least 3 emergency conditions that could be causing this patient’s symptoms. These can be documented as relevant conditions that you think the patient does NOT have, as well as things that you are considering and therefore need to be worked-up.
The physician is only able to clearly show that he thought of 2 possible causes: acute coronary syndrome and sunburn. There is room for improvement here. If he did not think the patient had a pulmonary embolism, aortic dissection, pneumothorax, pneumonia, or other emergency causes of chest pain, he should have documented his thoughts.
Discrepancies: None
Aftercare: 2/4
Aftercare consists of three main elements: plan of care, follow-up instructions, and return precautions. Each of these elements need specific timing. The plan of care in this case was to use topical Voltaren (a prescription was written). She was given vague instructions to follow-up with her primary care doctor, although without specific timeline and no real sense of urgency. Return precautions were not addressed.
The medical decisions made in this case were poor (rapid follow-up was not clearly recommended, and there was seemingly no effort to facilitate her care in the community where she was vacationing). The lack of documentation regarding these issues compounded the issue, and made the decisions even harder to defend.
Take-home points:
– Don’t assume the most benign explanation of a patient’s symptoms.
– Response to nitroglycerin is not a valid way to rule out cardiac ischemia.
– Ignore automated EKG interpretations.
– Ignore attorneys who want to talk about automated EKG interpretations.
– Document a differential of at least 3 items.
– Make sure the patient understands their follow-up instructions and return precautions.