A 47-year-old woman presented to the ED on November 6 with abdominal pain. The patient had undergone a Roux-en-Y gastric bypass surgery on October 20. She had developed worsening abdominal pain, and went to see a nurse practitioner at an outpatient clinic. She was given Rocephin and Phenergan, and then referred to the ED.
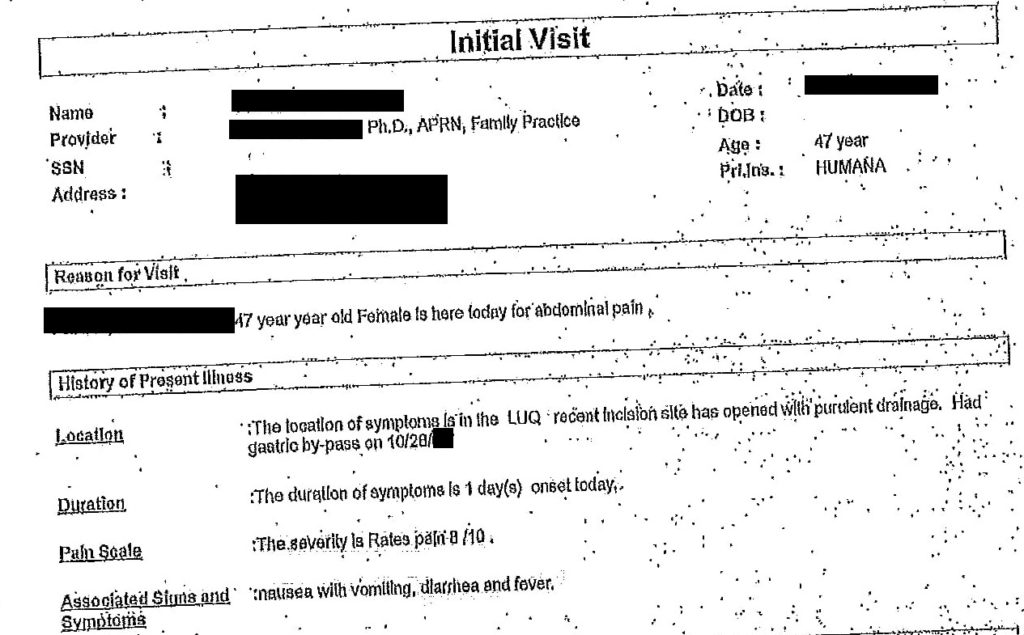


On arrival to the ED, the patient was seen by a physician. The T-sheet is shown below. The copies entered in the trial for this case are of particularly poor quality, therefore a summary of the information is shown below. The chief complaint is left abdominal wall abscess/drainage. Onset was today. Context: bypass on 10/20, now with incisional infection and drainage at L upper abdomen. A set of vitals revealed a temperature of 100.3 F, BP 141/74, HR 114, respirations 28/min, 100% O2 sat. The patient was noted to be in moderate distress. She had ecchymosis on her right side with a drain, the incision had purulent material and there was surrounding cellulitis. A CT with contrast was ordered to rule out abscess. An IV was started, she was given 1L NS bolus, several doses of morphine and Zofran.
Chemistry:
| Glucose | 98 mg/dL |
| BUN | 7 mg/dL |
| Creatinine | 0.6 mg/dL |
| Sodium | 134 mmol/L (L) |
| Potassium | 3.2 mmol/L (L) |
| Chloride | 96 mmol/L (L) |
| CO2 | 22 mmol/L |
| Calcium | 9.1 mg/dL |
| Anion Gap | 19 mmol/L (H) |
| GFR estimated | 114 mL/min |
CBC:
| WBC | 15.9 K/uL(H) |
| RBC | 4.16 mil/dL (L) |
| HGB | 11.7 g/dL (L) |
| HCT | 35.1% (L) |
| MCV | 84.4 fl |
| MCH | 28.2 pg |
| MCHC | 33.4 g/dL |
| Platelets | 494 K/uL (H) |
| Differential | |
| NEUT | 70.9% (H) |
| LYMP | 20.6% (L) |
| MONO | 6.1% |
| EOS | 0.7% |
| BASO | 1.7% |
| ABS NEUT | 11.3% (H) |
| ABS LYMPH | 3.3% |
| ABS MONO | 1.0% (H) |
| ABS EOS | 0.1% |
| ABS BASO | 0.1% (H) |
A CT scan was ordered. The results are below.
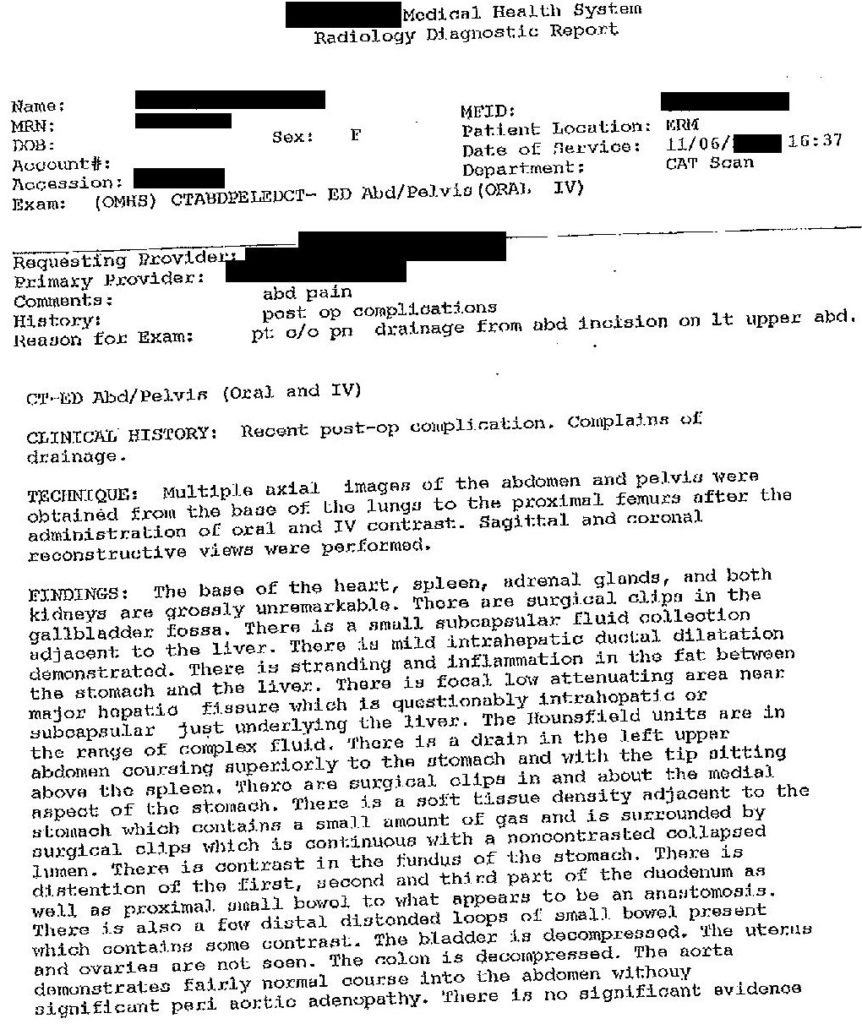
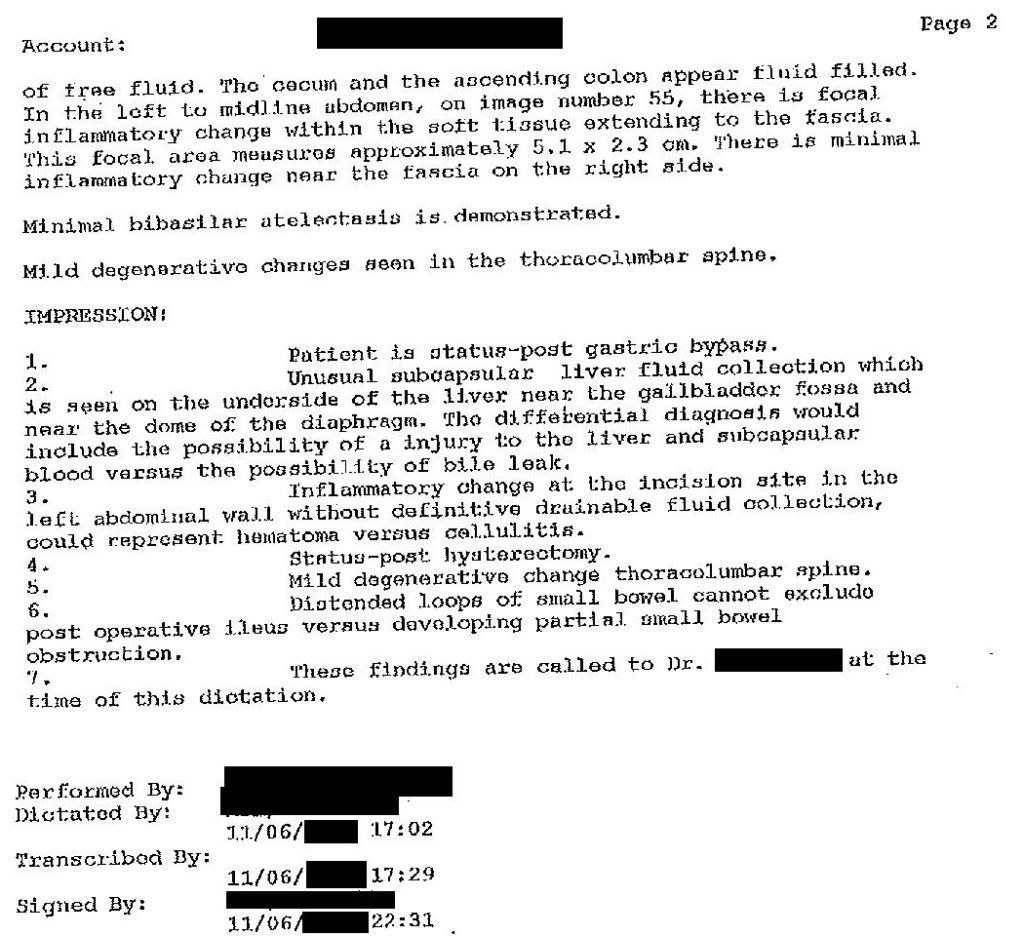
Given this information, what would be the appropriate next steps? Can this patient be discharged?